Two Dead, Eleven Critical: Fast-Moving Meningitis Outbreak Strikes University of Kent
An "invasive" meningitis cluster has killed two people aged 18-21 and left 11 others in serious condition in Canterbury. Health authorities have launched a mass antibiotic campaign and contacted more than 30,000 students, staff and their families. The strain has not yet been identified.
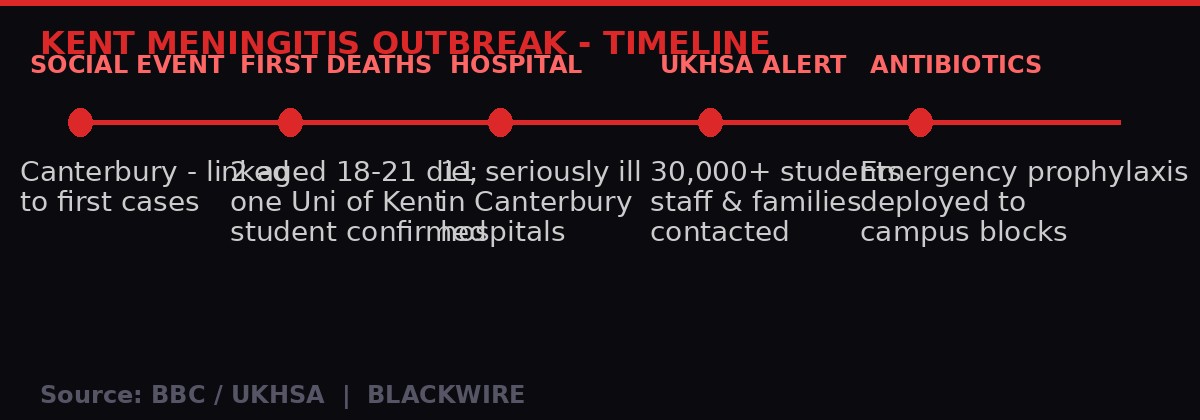
Outbreak timeline - University of Kent meningitis cluster, March 2026. Source: BBC / UKHSA / BLACKWIRE
What Happened
Two young people are dead and eleven more are fighting for their lives after an outbreak of "invasive" meningitis swept through the Canterbury area over the weekend, centred on the University of Kent campus. Both fatalities are believed to be aged between 18 and 21. The University confirmed that one of the two was a registered student.
The UK Health Security Agency (UKHSA) confirmed on Sunday evening that it had mobilised an emergency response, contacting more than 30,000 students, staff and family members to inform them of the outbreak and urging anyone with symptoms to seek immediate care. Specialists are conducting urgent contact tracing interviews with those who fell ill.
The outbreak is believed to be linked to a social event held in Canterbury, which investigators think was the common thread connecting the initial cases. The precise venue and date of that event are still being established by UKHSA epidemiologists.
A letter from the UKHSA, seen by the BBC, told students and staff living and working in specific campus residential blocks to receive antibiotics "without delay" as a precautionary measure. This prophylactic deployment - treating people before they show symptoms - is standard public health protocol when a bacterial meningitis cluster is confirmed in a closed community.
"The safety of our students and staff remains our highest priority. We are working closely with public health teams and are in touch with staff and students to ensure they get the advice and support they need." - University of Kent spokesperson, March 15, 2026
Canterbury MP Rosie Duffield described the deaths as "really tragic" in a post on X on Sunday night, saying she was "thinking very much" of those close to the victims. Kent County Council and local NHS trusts are working alongside UKHSA in the response.
Why University Campuses Are High-Risk Environments
Meningitis bacteria do not need a dramatic vector to spread. They live in the throats and nasal passages of roughly 10% of healthy adults at any given time without causing illness. They transmit through ordinary close-contact activities: coughing, sneezing, sharing drinks, kissing. University campuses compress thousands of people from different geographic backgrounds into shared accommodation, lecture halls and social spaces - exactly the environment where that 10% carriage rate can tip into an outbreak.
This is well understood by public health officials. The NHS MenACWY vaccine programme was specifically designed to address this risk, targeting teenagers before they arrive at university. All students starting university as "freshers" are offered the MenACWY jab, which covers four strains of meningococcal disease - Meningococcal A, C, W and Y. The MenB vaccine, covering the most common UK strain of bacterial meningitis, is offered to infants but is not currently part of the routine adolescent programme.
The critical unknown right now is which strain is responsible for the Kent outbreak. UKHSA confirmed on Sunday that the specific strain had not yet been identified. That matters enormously for two reasons. First, it determines whether the cases are vaccine-preventable under current UK immunisation schedules, and therefore whether a vaccination gap may have played a role. Second, it informs which antibiotics are most appropriate as prophylaxis for close contacts.
If the strain turns out to be MenB - the most common cause of bacterial meningitis in UK young people - the NHS would face a hard question: why is the routine MenB vaccine not offered to university students as it is to infants? Health advocates have lobbied for years to extend MenB coverage to adolescents and young adults, arguing that the protection from the infant dose wanes before peak university risk years.
"University students and young adults are among the groups at increased risk because meningitis bacteria can spread more easily in settings where people live, study and socialise closely together. We urge students, staff and families to remain vigilant for the signs and symptoms of meningitis." - Dr Tom Nutt, Chief Executive, Meningitis Now
The Race Against Time: How Bacterial Meningitis Kills
What makes this outbreak terrifying - and what public health officials are fighting against - is speed. Bacterial meningitis can move from first symptom to death in under 24 hours. The bacteria, typically Neisseria meningitidis (meningococcus) or Streptococcus pneumoniae (pneumococcus), can trigger a runaway inflammatory response once they breach the blood-brain barrier.
The early symptoms are almost impossible to distinguish from a bad flu or even a severe hangover - fever, headache, nausea. This overlap is particularly dangerous in university settings. Trish Mannes, UKHSA regional deputy director for the South East, acknowledged this directly.
"Students can be at risk of missing symptoms due to being easily confused with other illnesses such as a bad cold, flu or even a hangover." - Trish Mannes, UKHSA Regional Deputy Director, South East
As infection progresses, more distinctive symptoms can emerge: severe neck stiffness making it painful to bring the chin to the chest, extreme sensitivity to light, and - in the case of bacterial meningococcal septicaemia (blood poisoning) - a characteristic rash of small red or purple spots that do not fade when pressed with a glass. That "glass test" rash is a late-stage warning sign indicating bacteria have entered the bloodstream. By the time the rash appears, the patient is often critically ill.
Standard treatment requires immediate high-dose intravenous antibiotics, typically penicillin or ceftriaxone, along with IV fluids and often corticosteroids to reduce brain swelling. Every hour without treatment in a confirmed bacterial case significantly worsens outcomes. Up to one in ten confirmed bacterial meningitis cases in the UK is fatal even with treatment. Among those who survive, roughly a third are left with lasting complications including hearing loss, neurological damage, limb amputation, and severe scarring from skin necrosis.
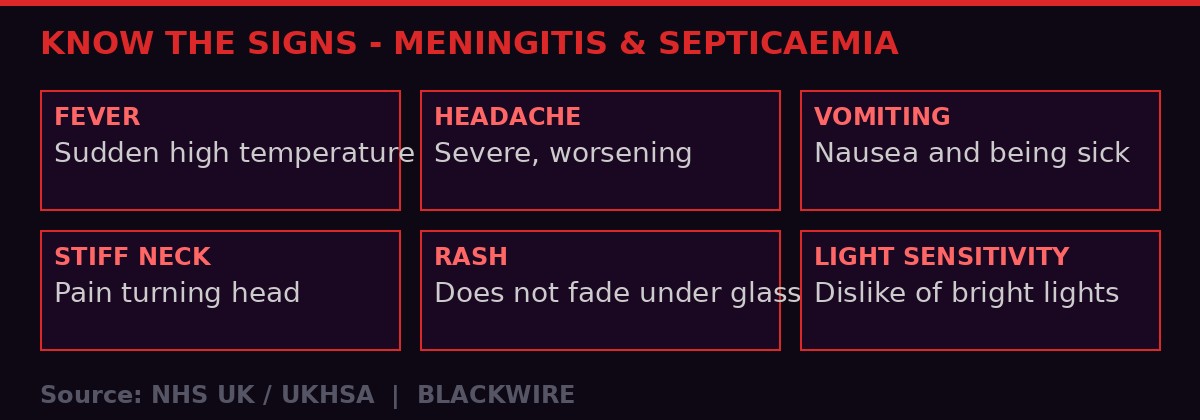
Critical warning signs of meningitis and meningococcal septicaemia. Source: NHS UK / UKHSA - BLACKWIRE
Emergency - Know These Symptoms Now
- Sudden high fever - appearing rapidly, often with sweating and chills
- Severe, worsening headache - unlike any normal headache
- Stiff neck - difficulty bringing chin to chest
- Vomiting and nausea, often accompanying the headache
- Sensitivity to light - eye pain or discomfort in bright light
- Rash that does not fade when a glass is pressed against it (red, purple spots) - this is a late-stage emergency
- Drowsiness, confusion, or difficulty waking
- Seizures in severe cases
Call 999 immediately or go to A&E. Do not wait for all symptoms. Do not wait for the rash. Trust your instincts.
The Public Health Response: 30,000 Contacted, Antibiotics Deployed
The UKHSA response is large by any standard. Contacting 30,000 people within hours of confirming a cluster outbreak signals that health authorities have assessed the risk as serious and escalating. The agency is not just reassuring people - it is actively distributing prophylactic antibiotics to close contacts of confirmed cases and to residents of specific campus buildings where exposure risk is judged to be highest.
Prophylaxis in meningitis outbreaks typically involves a short course of rifampicin, ciprofloxacin, or a single injection of ceftriaxone. These do not provide lasting protection - they clear the bacteria from the nose and throat before it has a chance to invade. The window for effective prophylaxis is short: it needs to be administered within days of exposure, ideally within 24 hours.
The fact that UKHSA issued instructions for antibiotics to be given "without delay" to residents of certain campus blocks suggests they have mapped the likely transmission chain and identified buildings as linked to the social event where initial spread is thought to have occurred. The epidemiological investigation is now focused on identifying every person who was at that event, and every close contact of those individuals.
The mass notification operation - texting and emailing 30,000+ people - requires coordinating between the university's student records, NHS patient data, and UKHSA regional systems. This kind of rapid data mobilisation became significantly more practised during COVID-19, and the infrastructure built during that pandemic is now being deployed for a different pathogen.
It is worth being clear about what prophylaxis does and does not do. It reduces the chance that a currently healthy person who may have been exposed will go on to develop the disease. It does not treat anyone who is already symptomatic. The eleven people currently in serious condition in Canterbury hospitals are beyond the prophylaxis stage - they are in the acute treatment phase, fighting for survival.
Historical Context: University Meningitis Outbreaks in the UK
The UK has a grim institutional memory of campus meningitis outbreaks. The scale of public fear they generate, combined with the speed of transmission in enclosed communities, has prompted multiple policy reviews and vaccination expansions over the past three decades.
In the late 1990s and early 2000s, meningococcal C disease was rising sharply in UK teenagers and young adults. A series of deaths at universities and secondary schools drove the introduction of the Men C vaccine into the childhood immunisation schedule in 1999 - one of the fastest vaccine rollouts in NHS history at that time. The introduction of Men C vaccination led to a dramatic reduction in Group C meningococcal disease in the UK, demonstrating that the vaccination approach works.
The 2015 introduction of the MenACWY vaccine for teenagers and university freshers followed a rise in Group W meningococcal disease, a strain that had been circulating in South American Hajj pilgrims and eventually seeded into UK communities. Group W is particularly associated with high case fatality rates compared to other strains. That vaccination push was again partly driven by documented campus deaths.
More recently, the introduction of the MenB vaccine for infants in 2015 was championed in part by families of young children who died from the disease. Since then, pressure has grown from charities like Meningitis Now and Meningitis Research Foundation for the MenB programme to be extended to older age groups, particularly the 15-24 bracket where risk is known to be elevated.
The Kent outbreak will inevitably reignite that debate. If the strain turns out to be MenB - which causes around 60% of all bacterial meningitis cases in UK teenagers and young adults - the policy gap becomes impossible to ignore. Students at the University of Kent who received the MenB jab as infants in 2015 or later are now around 10-11 years old. Those who are 18-21 today received the vaccine before it existed as a routine programme - most will have no MenB protection at all.
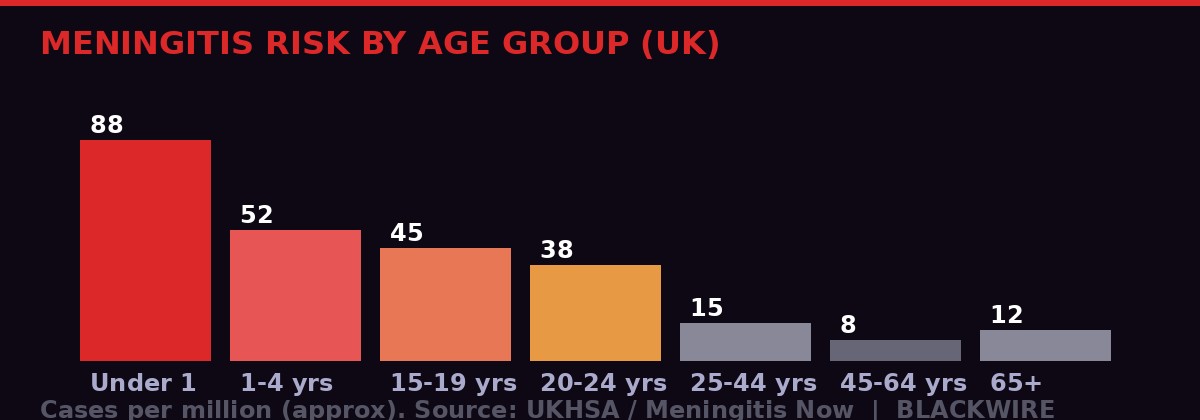
Approximate meningitis incidence by age group (UK data). University-age 15-24 bracket shows elevated risk. Source: UKHSA / Meningitis Now - BLACKWIRE
The University Under Pressure: What Kent Must Do Now
The University of Kent is one of England's mid-tier universities, with around 16,000 students based primarily on its Canterbury campus - a classic 1960s plate glass university set on a hill above the city. The campus architecture concentrates students in shared halls of residence, communal kitchens, and large social spaces. That layout, designed to foster community, is exactly the kind of environment where respiratory-transmitted bacteria find easy passage.
The institution is now in full crisis management mode. Beyond the immediate cooperation with UKHSA on contact tracing and antibiotic deployment, university leadership faces a set of decisions that have no clean answer. Do they cancel social events and sporting fixtures? Do they close residential buildings pending environmental sampling? Do they send students home - and if so, do they risk those students carrying bacteria back to their home communities?
These are not hypothetical questions. They are being actively discussed right now. The UKHSA response so far has been focused, not panicked - targeted buildings, identified close contacts, prophylaxis for the highest-risk individuals. A full campus closure is not currently indicated based on what is publicly known. But if the case count rises, or if the strain turns out to be a highly virulent variety with a broad exposure network, that calculus changes.
The university's student union has been working overnight to disseminate information. Students are being urged not to dismiss symptoms as a hangover, not to wait to see if they feel better in the morning, and not to be embarrassed about presenting to A&E with what might turn out to be a minor illness. In meningitis, the cost of a false alarm is a wasted afternoon in A&E. The cost of dismissing a real symptom can be death.
The university's counselling and mental health services are also now under considerable pressure. For a student body of 16,000-plus, the knowledge that two of their peers died this weekend - possibly someone they knew, possibly someone who was at the same event they attended - is a significant collective trauma. Managing both the physical outbreak and the psychological response is a dual challenge that the university's welfare infrastructure was not designed to handle simultaneously at this scale.
What Comes Next: Strain ID, Vaccine Review, Policy Questions
The most urgent piece of missing information is the meningococcal strain. UKHSA laboratory analysis is underway, and results on strain identification typically come within 24-72 hours of sample collection from confirmed cases. The moment that result is known, two things happen simultaneously: public health authorities can make a definitive assessment of how much risk the current UK immunisation schedule should have prevented, and the media and political temperature will spike accordingly.
If the strain is MenACWY - covered by the vaccine offered to all UK students as freshers - the question becomes vaccine uptake. What percentage of the affected students had actually received the MenACWY jab? Uptake of the fresher vaccination programme has historically been lower than the childhood schedule, in part because it requires students to actively seek the vaccine through GP registration rather than receiving it through a school-based programme.
If the strain is MenB - not covered by anything offered to this age group routinely - the political debate will be immediate and loud. Meningitis Now and the Meningitis Research Foundation have both lobbied for years for an extended MenB programme. Health economists have argued that the cost of vaccinating the full adolescent population does not meet NICE's standard cost-effectiveness thresholds. That argument is about to be stress-tested against the political reality of two dead teenagers and eleven more in hospital.
The Starmer government, already under pressure from the Iran-war-driven energy crisis dominating this Monday morning's news, has two simultaneous public health stories to manage - the Kent outbreak and the downstream effects of heating oil price gouging on vulnerable households. Health Secretary Wes Streeting has not yet made a public statement as of Monday morning. That silence will not last long.
In the immediate term, anyone in Canterbury or who has recently been on the University of Kent campus, attended social events in the area over the past two weeks, or knows someone who has - should monitor themselves for symptoms. If any of the warning signs listed above appear, the instruction from every health authority is the same: do not wait, do not self-diagnose, call 999 or go straight to A&E.
"Meningitis can progress very quickly and its impact is devastating, particularly for young people and their loved ones." - Dr Tom Nutt, Meningitis Now, March 2026
Two families in Canterbury are now planning funerals for their children. Eleven sets of parents are sitting by hospital bedsides. Thirty thousand people opened a text or email this weekend and felt their stomach drop. The next 72 hours - while strain results come in, while the case count either holds or climbs, while health officials work through contact lists - will define how large this outbreak becomes and what it forces policymakers to confront.
Meningitis: The Basics Everyone Needs to Know
Meningitis is an infection of the meninges - the protective membranes that surround the brain and spinal cord. It can be caused by bacteria, viruses, or in rare cases fungi. Bacterial meningitis is the dangerous kind: without rapid treatment, it can kill within hours.
The most common bacterial causes in UK young people are Neisseria meningitidis (meningococcal disease, multiple strains including B, C, W and Y) and Streptococcus pneumoniae (pneumococcal disease). Viral meningitis, usually caused by enteroviruses, is far more common but rarely fatal, typically resolving on its own within 7-10 days.
Treatment for bacterial meningitis requires hospital admission and IV antibiotics. The earlier treatment begins, the better the outcome. The NHS target is to administer antibiotics within one hour of hospital arrival for suspected bacterial meningitis cases.
Long-term complications from bacterial meningitis can include hearing loss, vision loss, cognitive difficulties, coordination problems, epilepsy, and - in the case of meningococcal septicaemia with purpura fulminans (the most severe rash presentation) - amputation of affected limbs due to tissue death caused by bacterial toxins in the bloodstream.
The UK vaccination schedule currently offers:
- MenB vaccine - for infants at 8 weeks, 12 weeks and 1 year. Covers Group B meningococcal disease, the most common UK strain.
- MenACWY vaccine - for teenagers (around age 14 via school programme) and for university freshers through GP registration. Covers Groups A, C, W and Y.
- Pneumococcal vaccine - part of childhood schedule and offered to adults 65+. Covers the most common pneumococcal strains.
The gap for university-age students is MenB. Anyone currently aged 18-21 who did not receive MenB as an infant (because the programme began in 2015) is effectively unvaccinated against the most common strain of bacterial meningitis. The Kent outbreak may force a public reckoning with whether that gap is acceptable.
Get BLACKWIRE reports first.
Breaking news, investigations, and analysis - straight to your phone.
Join @blackwirenews on TelegramSources: BBC News (Mark Norman, Patrick Barlow - March 15/16, 2026), UK Health Security Agency (UKHSA) official statement March 15, 2026, Meningitis Now (Dr Tom Nutt statement), NHS UK (meningitis clinical guidance), Canterbury MP Rosie Duffield (X/Twitter statement). This report will be updated as strain identification and case count information becomes available.